Overview
The condition is more common in young people active in sport, and boys are more frequently affected than girls. One study found the average age of presentation was around 12 years for boys and 9 years for girls. In one prospective study of injuries among players aged 9-19 years in football academies, 2% of overall football injuries were due to Sever's disease; the peak for incidence was in the under-11 age group. In a study of 85 children, the condition was bilateral in 61%.
Causes
Sever?s disease only occurs during a certain period of pre-adolescence, when the heel bone is going through a rapid growth spurt. In girls, this typically occurs around 8 to 10 years of age, and in boys, between ages 10 and 13. Sever?s disease is more common in active, athletic children. The condition is difficult to prevent completely, but changing the type and amount of physical activity when your child is experiencing pain will help.
Symptoms
Athletes with Sever?s disease are typically aged 9 to 13 years and participate in running or jumping sports such as soccer, football, basketball, baseball, and gymnastics. The typical complaint is heel pain that develops slowly and occurs with activity. The pain is usually described like a bruise. There is rarely swelling or visible bruising. The pain is usually worse with running in cleats or shoes that have limited heel lift, cushion, and arch support. The pain usually goes away with rest and rarely occurs with low-impact sports such as bicycling, skating, or swimming.
Diagnosis
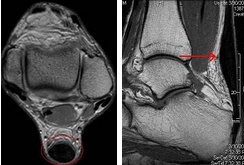
Sever condition is diagnosed by detecting the characteristic symptoms and signs above in the older children, particularly boys between 8 and 15 years of age. Sometimes X-ray testing can be helpful as it can occasionally demonstrate irregularity of the calcaneus bone at the point where the Achilles tendon attaches.
Non Surgical Treatment
Orthotic insoles are a common form of treatment for Sever?s disease as they provide support and cushioning to the area which reduces the pressure and stress to the area. Our podiatrist can also show your child stretches and exercises to help them manage their pain as well offering them advice on their exercise and activity.
Surgical Treatment
The surgeon may select one or more of the following options to treat calcaneal apophysitis. Reduce activity. The child needs to reduce or stop any activity that causes pain. Support the heel. Temporary shoe inserts or custom orthotic devices may provide support for the heel. Medications. Nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, help reduce the pain and inflammation. Physical therapy. Stretching or physical therapy modalities are sometimes used to promote healing of the inflamed issue. Immobilization. In some severe cases of pediatric heel pain, a cast may be used to promote healing while keeping the foot and ankle totally immobile. Often heel pain in children returns after it has been treated because the heel bone is still growing. Recurrence of heel pain may be a sign of calcaneal apophysitis, or it may indicate a different problem. If your child has a repeat bout of heel pain, be sure to make an appointment with your foot and ankle surgeon.
The condition is more common in young people active in sport, and boys are more frequently affected than girls. One study found the average age of presentation was around 12 years for boys and 9 years for girls. In one prospective study of injuries among players aged 9-19 years in football academies, 2% of overall football injuries were due to Sever's disease; the peak for incidence was in the under-11 age group. In a study of 85 children, the condition was bilateral in 61%.
Causes
Sever?s disease only occurs during a certain period of pre-adolescence, when the heel bone is going through a rapid growth spurt. In girls, this typically occurs around 8 to 10 years of age, and in boys, between ages 10 and 13. Sever?s disease is more common in active, athletic children. The condition is difficult to prevent completely, but changing the type and amount of physical activity when your child is experiencing pain will help.
Symptoms
Athletes with Sever?s disease are typically aged 9 to 13 years and participate in running or jumping sports such as soccer, football, basketball, baseball, and gymnastics. The typical complaint is heel pain that develops slowly and occurs with activity. The pain is usually described like a bruise. There is rarely swelling or visible bruising. The pain is usually worse with running in cleats or shoes that have limited heel lift, cushion, and arch support. The pain usually goes away with rest and rarely occurs with low-impact sports such as bicycling, skating, or swimming.
Diagnosis
Sever condition is diagnosed by detecting the characteristic symptoms and signs above in the older children, particularly boys between 8 and 15 years of age. Sometimes X-ray testing can be helpful as it can occasionally demonstrate irregularity of the calcaneus bone at the point where the Achilles tendon attaches.
Non Surgical Treatment
Orthotic insoles are a common form of treatment for Sever?s disease as they provide support and cushioning to the area which reduces the pressure and stress to the area. Our podiatrist can also show your child stretches and exercises to help them manage their pain as well offering them advice on their exercise and activity.
Surgical Treatment
The surgeon may select one or more of the following options to treat calcaneal apophysitis. Reduce activity. The child needs to reduce or stop any activity that causes pain. Support the heel. Temporary shoe inserts or custom orthotic devices may provide support for the heel. Medications. Nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, help reduce the pain and inflammation. Physical therapy. Stretching or physical therapy modalities are sometimes used to promote healing of the inflamed issue. Immobilization. In some severe cases of pediatric heel pain, a cast may be used to promote healing while keeping the foot and ankle totally immobile. Often heel pain in children returns after it has been treated because the heel bone is still growing. Recurrence of heel pain may be a sign of calcaneal apophysitis, or it may indicate a different problem. If your child has a repeat bout of heel pain, be sure to make an appointment with your foot and ankle surgeon.


 Achilles tendinitis is often a misnomer, as most problems associated with the Achilles tendon are not strictly an inflammatory response. A more appropriate term, which most experts now use, is Achilles tendinopathy which includes, Tendinosis, microtears in the tissues in and around the tendon. Tendinitis, inflammation of the tendon Most cases of Achilles tendon pain is the result of tendinosis. Tendon inflammation (tendinitis) is rarely the cause of tendon pain. Achilles tendinopathy is a common condition that occurs particularly in athletes and can be difficult to treat due to the limited vascular supply of the tendon and the stress within the Achilles tendon with every step. Evidence indicates that treatment incorporating custom foot orthoses can improve this condition by making the foot a more effective lever in gait. A 2008 study reported between 50 and 100% relief (average 92%) from Achilles tendinopathy symptoms with the use of custom foot orthoses.
Achilles tendinitis is often a misnomer, as most problems associated with the Achilles tendon are not strictly an inflammatory response. A more appropriate term, which most experts now use, is Achilles tendinopathy which includes, Tendinosis, microtears in the tissues in and around the tendon. Tendinitis, inflammation of the tendon Most cases of Achilles tendon pain is the result of tendinosis. Tendon inflammation (tendinitis) is rarely the cause of tendon pain. Achilles tendinopathy is a common condition that occurs particularly in athletes and can be difficult to treat due to the limited vascular supply of the tendon and the stress within the Achilles tendon with every step. Evidence indicates that treatment incorporating custom foot orthoses can improve this condition by making the foot a more effective lever in gait. A 2008 study reported between 50 and 100% relief (average 92%) from Achilles tendinopathy symptoms with the use of custom foot orthoses.
 Achilles tendinitis (tendonitis) or Achilles tendon inflammation occurs when the Achilles tendon becomes inflamed, as a result, of the Achilles tendon being put under too much strain. The Achilles tendon joins the calf muscles to the heel bone, and is found at the back of a person's lower leg. It is the largest tendon in the body and can endure great force, but is still susceptible to injury. Achilles tendinitis is usually the result of strenuous, high impact exercise, such as running. If ignored, Achilles tendinitis can lead to the tendon tearing or rupturing, and therefore it is important to seek the necessary treatment. Sometimes, treatment can be as simple as getting rest or changing an exercise routine. However, in more severe cases, surgery may be required.
Achilles tendinitis (tendonitis) or Achilles tendon inflammation occurs when the Achilles tendon becomes inflamed, as a result, of the Achilles tendon being put under too much strain. The Achilles tendon joins the calf muscles to the heel bone, and is found at the back of a person's lower leg. It is the largest tendon in the body and can endure great force, but is still susceptible to injury. Achilles tendinitis is usually the result of strenuous, high impact exercise, such as running. If ignored, Achilles tendinitis can lead to the tendon tearing or rupturing, and therefore it is important to seek the necessary treatment. Sometimes, treatment can be as simple as getting rest or changing an exercise routine. However, in more severe cases, surgery may be required.



 Plantar Fasciitis is an inflammation caused by excessive stretching of the plantar fascia. The plantar fascia is a broad band of fibrous tissue which runs along the bottom surface of the foot, attaching at the bottom of the heel bone and extending to the forefoot. When the plantar fascia is excessively stretched, this can cause plantar fasciitis, which can also lead to heel pain, arch pain, and heel spurs.
Plantar Fasciitis is an inflammation caused by excessive stretching of the plantar fascia. The plantar fascia is a broad band of fibrous tissue which runs along the bottom surface of the foot, attaching at the bottom of the heel bone and extending to the forefoot. When the plantar fascia is excessively stretched, this can cause plantar fasciitis, which can also lead to heel pain, arch pain, and heel spurs. Plantar fasciitis usually develops slowly, although in some cases the pain can appear instantly and be very intense. Symptoms of plantar fasciitis include Sharp, stabbing pain in the inside bottom part of the heel, Pain worsens as you stand, climb, tiptoe, etc., Pain is worse after long periods of rest, or first thing in the morning, Pain increases over a period of months, Not much pain while moving around, but an aching feeling after sitting down, Sometimes sufferers will feel pain when they walk, run, or jog. Other times, the pain will not be noticeable until they slow down and relax, possibly even after waking up from a good night?s sleep. If you are experiencing any of these symptoms, you should consider seeing a podiatrist before the problem worsens.
Plantar fasciitis usually develops slowly, although in some cases the pain can appear instantly and be very intense. Symptoms of plantar fasciitis include Sharp, stabbing pain in the inside bottom part of the heel, Pain worsens as you stand, climb, tiptoe, etc., Pain is worse after long periods of rest, or first thing in the morning, Pain increases over a period of months, Not much pain while moving around, but an aching feeling after sitting down, Sometimes sufferers will feel pain when they walk, run, or jog. Other times, the pain will not be noticeable until they slow down and relax, possibly even after waking up from a good night?s sleep. If you are experiencing any of these symptoms, you should consider seeing a podiatrist before the problem worsens. RSS Feed
RSS Feed
